


“What is the most effective medication for prostatitis?” is probably the most common question asked by men suffering from perineal pain, urinary burning, pelvic discomfort, or sexual dysfunction. Many patients are looking for a simple answer, hoping to find a pill capable of permanently eliminating the problem.
The clinical reality, however, is very different, because there is no single medication that is best for all forms of prostatitis. The most effective treatment heavily depends on the specific clinical form, the presence or absence of bacteria, the degree of inflammation, the presence of chronic pain, and the individual characteristics of each patient. This perfectly explains why a medication that is extremely effective in some men may be completely ineffective in others.
Quick Answer
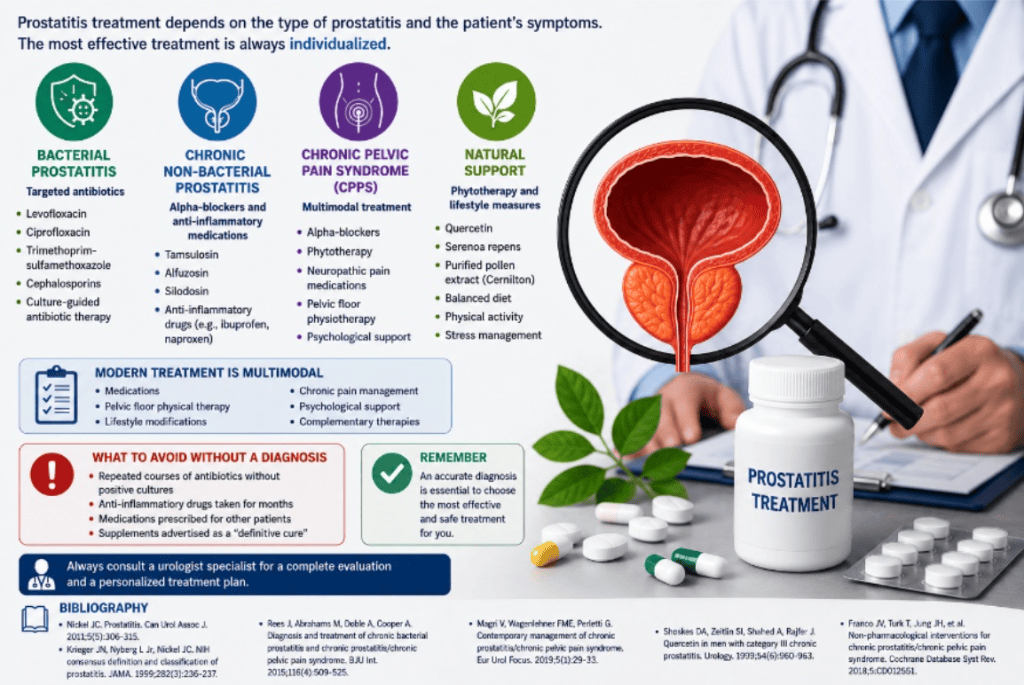
If you are looking for a direct answer to the question, “What is the most effective medication for prostatitis?”, the correct response is that in bacterial prostatitis, antibiotics are undoubtedly the most effective treatment; specifically, in chronic bacterial prostatitis, antibiotics with high prostatic penetration are required.
In contrast, in chronic non-bacterial prostatitis, antibiotics are often not the solution. The same applies to Chronic Pelvic Pain Syndrome (CPPS), where the most effective treatment is generally multimodal and may include pelvic floor physical therapy, alpha-blockers, antispasmodic medications, and drugs effective against pudendal neuropathy. Therefore, the first and most important question should not be which medication to use, but rather which type of prostatitis is present.
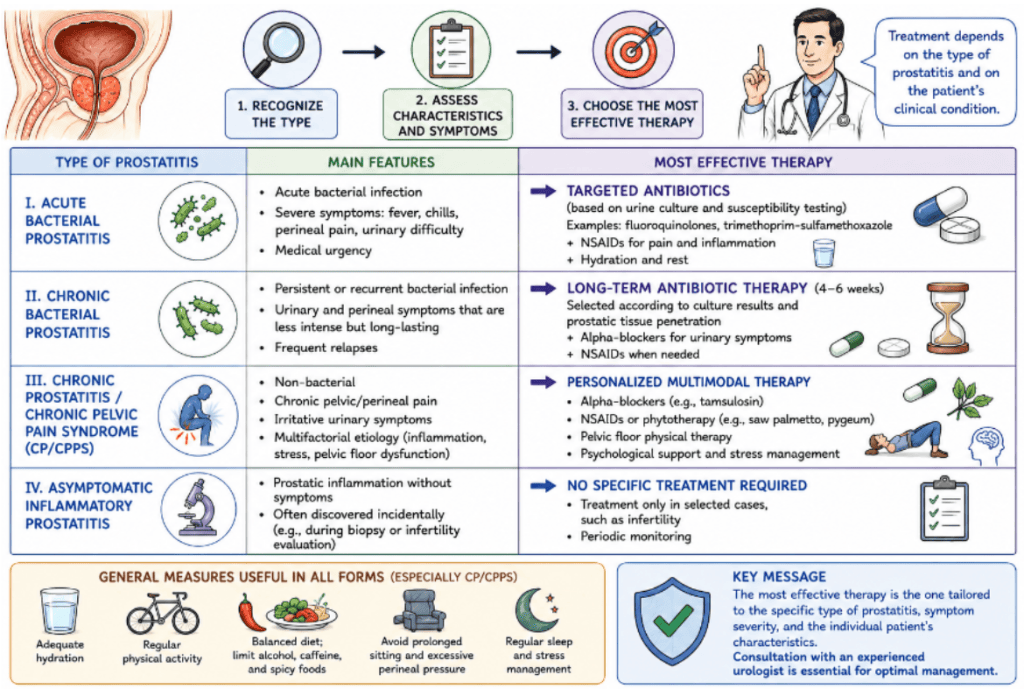
According to the National Institutes of Health (NIH), prostatitis is classified into four distinct categories. These include acute bacterial prostatitis and chronic bacterial prostatitis. The third category is Chronic Pelvic Pain Syndrome (CPPS), which alone accounts for approximately 90–95% of chronic prostatitis diagnoses and is often not associated with any demonstrable infection. Finally, the classification includes asymptomatic inflammatory prostatitis.
What Is the Most Effective Treatment for the Different Forms of Prostatitis?
The therapeutic approach varies significantly based on the clinical picture. For acute bacterial prostatitis, targeted antibiotics represent the most effective treatment, whereas chronic bacterial prostatitis strictly requires antibiotics with high prostatic penetration. Conversely, for CPPS, the best path forward is a multimodal therapy approach. Asymptomatic inflammatory prostatitis, on the other hand, typically requires no specific treatment.
What Is the Best Antibiotic for Bacterial Prostatitis?
This is undoubtedly one of the most common prostatitis-related searches on Google, but the truth is that there is no universally superior antibiotic. The best antibiotic is simply the one that is effective against the bacterium actually causing the infection. The microorganisms most frequently involved in these infections are enterobacteria, including Escherichia coli, Klebsiella species, Proteus species, and Enterococcus species.
For many years, Levofloxacin has been considered one of the reference treatments because of its excellent prostatic penetration and high effectiveness in susceptible infections. However, potential disadvantages include tendon-related adverse effects and increasing bacterial resistance. Ciprofloxacin achieves high concentrations within prostatic tissue and has long been used for bacterial prostatitis, but much like levofloxacin, it contributes to antimicrobial resistance and may cause significant gastrointestinal side effects.
Fosfomycin, in recent years, has gained increasing importance in clinical practice. Several studies have demonstrated promising results, particularly in treating infections caused by multidrug-resistant bacteria, and it is also generally well tolerated by patients. Finally, Trimethoprim-sulfamethoxazole (commonly known as Bactrim) may be effectively used in selected patients with documented infections caused by susceptible organisms.
Do Antibiotics Always Work?
No, they don’t, and this is probably the greatest misconception regarding prostatitis treatment. Many patients receive repeated courses of antibiotics without any documented evidence of bacterial infection. The European Association of Urology (EAU) guidelines clearly emphasize that prolonged antibiotic use in the absence of proven infection is not only discouraged but generally completely ineffective.
What Is the Most Effective Medication for Chronic Prostatitis?
In the realm of chronic non-bacterial prostatitis, the therapeutic answer changes completely. Many patients do not improve with antibiotics simply because the underlying problem is not an infection. Depending on the precise diagnosis, treatment in these scenarios may successfully include alpha-blockers, anti-inflammatory medications, pelvic floor physical therapy, and neuropathic pain management.
Alpha-blockers are highly valuable as they improve urinary symptoms, especially obstructive ones, by relaxing the bladder neck and prostatic smooth muscle. They are among the most effective medications for urinary issues, and common alpha-blockers include Tamsulosin, Alfuzosin, Silodosin, and Doxazosin. These medications may significantly improve urinary frequency, calm urinary urgency, and resolve issues like a weak urinary stream and incomplete bladder emptying. According to several clinical studies, a significant number of patients obtain notable improvements in their quality of life thanks to these drugs.
Anti-inflammatory medications can be very useful, but specifically in patients with a significant inflammatory component, helping to effectively reduce perineal pain, pelvic pain, urinary burning, and post-ejaculatory pain.
Regarding neuropathic pain medications, which are crucial in CPPS, the drugs most commonly used in clinical practice include Pregabalin, Gabapentin, Amitriptyline, and Duloxetine. These drugs do not eliminate the prostatitis itself but can significantly reduce chronic pain symptoms.
In clinical experience, there is no single standard therapy that works for every patient. In men with documented infection, targeted antibiotic therapy remains the absolute cornerstone of treatment. In patients with CPPS, however, particular attention is paid not only to pelvic floor physical therapy and pain control, but also to the improvement of urinary function. The primary goal becomes the reduction of pelvic muscle tension, which often leads to decreased irritation of the pudendal nerves. In fact, many men with CPPS present with pelvic floor hypertonicity and marked tenderness of myofascial trigger points resulting directly from chronic muscular contraction.
What Do the European Association of Urology Guidelines Recommend?
The EAU guidelines primarily emphasize the need for an accurate diagnosis before initiating any treatment, precisely to avoid the unnecessary and potentially harmful use of antibiotics. They strongly recommend a multimodal approach based on a thorough pelvic floor assessment, and they advocate for highly individualized management strategies to achieve effective chronic pain control.
Modern guidelines have completely abandoned the outdated concept that all forms of prostatitis are infectious and therefore require antibiotics. Consequently, among the most important mistakes to avoid are taking antibiotics without culture-based evidence of infection, a practice that paves the way for antimicrobial resistance and delays the correct diagnosis. Engaging in self-medication and searching for elusive “miracle cures” online are equally discouraged. Chronic prostatitis syndromes are complex, multifaceted conditions that rarely have simplistic solutions.
Frequently Asked Questions (FAQ)
What is the best antibiotic for prostatitis? It entirely depends on the causative bacterium and the results of the antibiotic susceptibility testing.
Is fosfomycin effective? Yes, it may be particularly useful, especially in infections caused by highly resistant bacteria.
Does tamsulosin cure prostatitis? No, it doesn’t cure the inflammation itself, but it can significantly improve troublesome urinary symptoms.
Is there a definitive cure? Once again, it depends on the specific type of prostatitis you are dealing with.
Do antibiotics always work? No. In non-bacterial forms, they are very often ineffective.
Can physical therapy be more effective than medications? Yes, in many patients suffering from CPPS, it absolutely can.
Can prostatitis increase PSA levels? Yes, prostatic inflammation may cause a temporary elevation of PSA.
Can prostatitis cause erectile dysfunction? Yes, particularly in the chronic forms of the condition.
Which supplements have the best evidence? Quercetin and Cernilton are among the most studied and promising supplements.
Does stress worsen prostatitis? Many studies strongly suggest a correlation between high stress levels and worsening symptoms.
Conclusions
There is no single, one-size-fits-all answer to the question, “What is the most effective medication for prostatitis?”. In bacterial prostatitis, antibiotics undoubtedly remain the most effective treatment. However, in chronic non-bacterial prostatitis and Chronic Pelvic Pain Syndrome, integrated approaches that intelligently combine medications, physical therapy, pain management, and specific lifestyle modifications are often far more effective.
The key to success is not obsessively searching for a miracle drug, but rather correctly identifying the true cause of the symptoms to develop, alongside a specialist, a highly personalized treatment plan.
Article reviewed by Prof. Federico Guercini, Specialist in Urology and Andrology.
Bibliografia
- Nickel JC. Prostatitis. Can Urol Assoc J. 2011;5(5):306-315.
- Krieger JN, Nyberg L Jr, Nickel JC. NIH consensus definition and classification of prostatitis. JAMA. 1999;282(3):236-237.
- Rees J, Abrahams M, Doble A, Cooper A. Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome. BJU Int. 2015;116(4):509-525.
- Magri V, Wagenlehner FME, Perletti G. Contemporary management of chronic prostatitis/chronic pelvic pain syndrome. Eur Urol Focus. 2019;5(1):29-33.
- Shoskes DA, Zeitlin SI, Shahed A, Rajfer J. Quercetin in men with category III chronic prostatitis. Urology. 1999;54(6):960-963.
- Franco JV, Turk T, Jung JH, et al. Non-pharmacological interventions for chronic prostatitis/chronic pelvic pain syndrome. Cochrane Database Syst Rev. 2018;5.
- Engeler D, Baranowski AP, Elneil S, et al. EAU Guidelines on Chronic Pelvic Pain. European Association of Urology. Latest edition.
- Pontari MA, Ruggieri MR. Mechanisms in prostatitis/chronic pelvic pain syndrome. J Urol. 2004;172(3):839-845.