


High PSA: Does It Always Mean Prostate Cancer?
Receiving a laboratory report showing a high PSA level is one of the most frightening situations for men over the age of 50. Many patients immediately associate an elevated PSA with prostate cancer, but reality is far more complex.
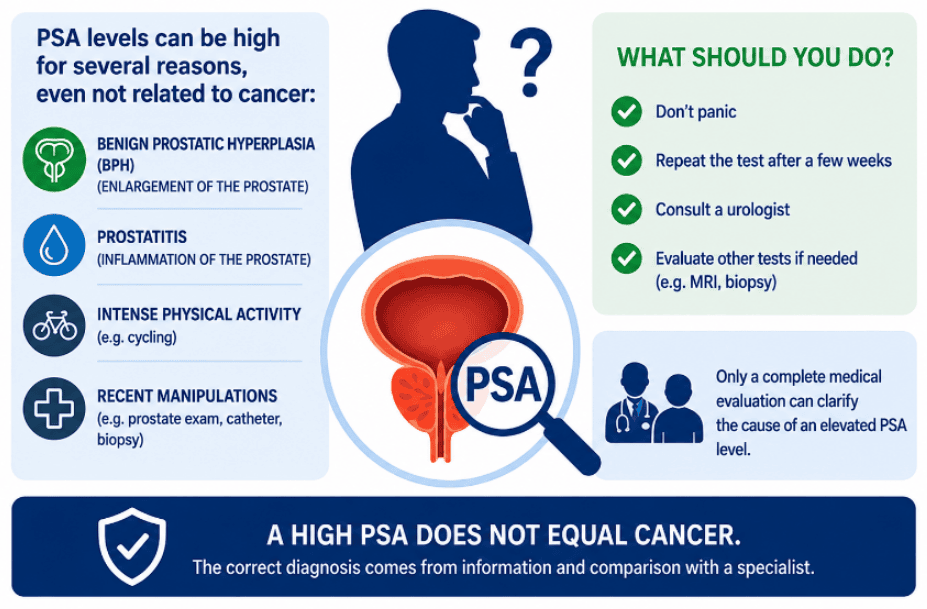
In most cases, a high PSA does not automatically indicate prostate cancer. Numerous benign conditions can increase PSA levels, including prostatitis, prostate inflammation, benign prostatic enlargement, and urinary tract infections.
Modern urology no longer interprets PSA as an isolated number. Instead, it is considered part of a comprehensive clinical assessment that includes:
- Urological examination
- Patient age
- Prostate volume
- PSA trend over time
- Multiparametric prostate MRI
- PSA density
- Family history of prostate cancer
Understanding the true significance of an elevated PSA is essential to avoid both unnecessary anxiety and dangerous underestimation of a potentially serious condition.
What Is PSA and Why Does It Increase?
PSA (Prostate-Specific Antigen) is a protein produced by the prostate gland.
Normally, a small amount of PSA enters the bloodstream and can be measured with a simple blood test. In most modern laboratories, the normal reference range is considered approximately 0–3.5 ng/mL.
The important point is that PSA levels increase not only because of prostate cancer.
PSA may also rise due to:
- Chronic prostatitis
- Prostate inflammation
- Benign prostatic hyperplasia (BPH)
- Urinary tract infections
- Recent ejaculation
- Recent transrectal urological examination
- Catheterization
- Urinary retention
- Prostate biopsy
- Intense physical activity
- Advanced age
For this reason, PSA is not a cancer-specific test but rather an indicator of prostate activity or distress.
High PSA: What Are the Normal Values?
Many men search online:
“What is a normal PSA level?”
In reality, there is no single PSA value that applies to everyone.
Traditionally:
- PSA below 3.5 ng/mL → generally considered normal
- PSA between 3.5 and 10 ng/mL → intermediate-risk zone
- PSA above 10 ng/mL → higher suspicion of prostate cancer
However, we now know that:
- Some men with low PSA levels still have prostate cancer.
- Many men with elevated PSA levels do not have cancer.
Therefore, several factors are crucial:
- Age
- Prostate size (PSA density)
- PSA trend over time (PSA velocity)
- Presence of prostatitis
- Family history
Elevated PSA Without Cancer: The Most Common Causes
Acute and Chronic Prostatitis
Prostatitis is one of the most common causes of elevated PSA.
Inflammation disrupts the prostate gland’s cellular barrier and facilitates the release of PSA into the bloodstream.
In acute prostatitis, PSA elevation typically shows:
- Sudden increase
- Very high values, sometimes exceeding 20 ng/mL
- Associated symptoms of acute prostatitis
In chronic prostatitis, which may present with milder or even silent symptoms, PSA elevations are usually more modest, often ranging up to approximately 6–7 ng/mL.
Many patients with chronic prostatitis experience fluctuating PSA levels over time.
Enlarged Prostate (Benign Prostatic Hyperplasia)
As men age, the prostate naturally increases in size.
A larger prostate produces more PSA.
Consequently, men with significantly enlarged prostates may have moderately elevated PSA levels without any evidence of prostate cancer.
In these cases, PSA density and PSA velocity become particularly important.
Urinary Tract Infections
Even a simple urinary tract infection may temporarily increase PSA levels.
Therefore, PSA testing should generally be avoided during active infections or febrile illnesses.
Recent Ejaculation
Ejaculation within the previous 24–48 hours may temporarily increase PSA levels.
Most specialists recommend sexual abstinence for at least 48 hours before PSA testing.
Does a High PSA Always Mean Prostate Cancer?
No.
This is perhaps the most important message.
Many men with abnormal PSA levels do not have prostate cancer.
Nevertheless, elevated PSA should never be ignored, especially when:
- PSA rises rapidly
- PSA exceeds certain thresholds
- There is a family history of prostate cancer
- Suspicious nodules are detected during imaging or rectal examination
- PSA density or PSA velocity is elevated
The modern goal of urology is to distinguish between:
- Benign conditions
- Indolent cancers
- Clinically significant aggressive cancers
PSA Density and PSA Velocity: Two Key Parameters
PSA density is one of the most useful tools in contemporary prostate cancer diagnostics.
It is calculated by dividing the PSA value by prostate volume.
PSA Density = PSA / Prostate Volume
A PSA density above 0.15 is generally considered suspicious for clinically significant prostate cancer.
This parameter helps distinguish:
- A large prostate producing an appropriate amount of PSA
- A PSA level disproportionately high for prostate size
PSA velocity refers to the rate of PSA increase over time.
A PSA velocity greater than 0.75 ng/mL per year is generally considered concerning.
Free PSA and Total PSA
The ratio between free PSA and total PSA may provide additional diagnostic information.
In many prostate cancers:
- Free PSA tends to decrease
- The free-to-total PSA ratio becomes lower
A low free PSA ratio increases suspicion for malignancy.
However, this parameter should always be interpreted within the broader clinical context.
A free-to-total PSA ratio below approximately 0.18 is commonly considered suspicious.
When Is Multiparametric Prostate MRI Necessary?
Multiparametric MRI (mpMRI), performed with intravenous contrast enhancement, has revolutionized prostate cancer diagnosis.
Today it often represents the most important step following an abnormal PSA result.
MRI can:
- Identify suspicious lesions
- Reduce unnecessary biopsies
- Estimate potential aggressiveness
- Improve diagnostic accuracy
Lesions are classified according to the PI-RADS v2.1 system:
- PI-RADS 1–2 → Low risk
- PI-RADS 3 → Intermediate risk
- PI-RADS 4–5 → High suspicion of clinically significant cancer
It is important to remember that the PI-RADS score itself does not establish the presence or absence of cancer. Rather, it helps the urologist determine whether a biopsy should be performed.
When Is a Prostate Biopsy Necessary?
A prostate biopsy is not automatically performed in every patient with elevated PSA.
The decision depends on:
- PSA value
- PSA density
- PSA velocity
- Digital rectal examination findings
- Multiparametric MRI findings
- Age
- Family history
- PSA trend over time
The most accurate biopsy technique currently available is MRI-ultrasound fusion biopsy.
This technique combines previously acquired MRI images with real-time transrectal ultrasound images.
Typically:
- 3–4 targeted cores are obtained from suspicious MRI lesions
- Additional systematic cores are obtained from other prostate regions
However, many centers still perform saturation biopsy or random systematic biopsy guided solely by ultrasound, obtaining approximately 20–26 tissue samples throughout the prostate.
What Symptoms Can Prostate Cancer Cause?
In its early and intermediate stages, prostate cancer often causes no symptoms.
In more advanced stages, symptoms may include:
- Difficulty urinating
- Blood in the urine
- Blood in the semen
- Bone pain in metastatic disease
The challenge is that many of these symptoms may also occur in benign prostate conditions.
Family History and Genetic Risk
A positive family history increases the risk of prostate cancer.
Particular attention is warranted in men with:
- A father diagnosed with prostate cancer
- One or more affected brothers
- BRCA mutations
- Multiple family members with cancer
In these individuals, PSA monitoring should generally begin before age 45.
Common Mistakes Made by Men with High PSA
1. Assuming the Worst Immediately
A high PSA does not automatically mean cancer.
2. Ignoring the Problem
An abnormal PSA always deserves evaluation.
3. Taking Unnecessary Antibiotics
Many patients receive antibiotic therapy without a clear indication.
4. Using Dutasteride Without Considering Its Effect on PSA
Dutasteride reduces intraprostatic androgen activity and is commonly prescribed for benign prostatic hyperplasia.
However, it artificially lowers PSA levels and may mask the presence of prostate cancer.
PSA testing should ideally be performed at least one month after discontinuation of the medication.
5. Repeating PSA Tests Too Frequently
Excessive testing often creates unnecessary anxiety.
6. Trusting Random Online Information
Every patient requires individualized evaluation.
PSA and Artificial Intelligence: The Future of Prostate Cancer Diagnosis
Artificial intelligence is rapidly entering prostate diagnostics.
AI systems can assist in:
- MRI interpretation
- PI-RADS assessment
- Cancer risk prediction
- Integration of PSA and imaging data
- Improving diagnostic accuracy
The future goal is increasingly personalized and less invasive prostate cancer care.
When Should You See a Urologist Promptly?
Prompt consultation with a urologist is recommended when:
- PSA remains persistently elevated
- PSA rises rapidly
- Significant family history is present
- Blood appears in the semen
- Severe urinary symptoms develop
Early evaluation leads to more accurate diagnosis and often less aggressive treatment.
Conclusion: What Does a High PSA Really Mean?
A high PSA does not automatically mean prostate cancer.
Many benign conditions may increase PSA levels, including:
- Prostatitis
- Enlarged prostate
- Prostate inflammation
- Urinary tract infections
Modern PSA interpretation relies on a comprehensive assessment that includes:
- Urological examination
- PSA density
- PSA velocity
- Multiparametric MRI
- PSA trend over time
- Individual risk profile
The goal is not merely to detect cancer, but to identify clinically significant cancers while avoiding unnecessary biopsies and overtreatment.
For this reason, an elevated PSA should always be interpreted by a physician experienced in prostate diseases.
Frequently Asked Questions (FAQ)
Does a high PSA always mean prostate cancer?
No. Many benign conditions can increase PSA levels.
Can prostatitis significantly increase PSA?
Yes, sometimes dramatically.
Can I have prostate cancer with a normal PSA?
Yes. Some prostate cancers occur despite low PSA levels.
When is prostate MRI recommended?
Often after an abnormal PSA result or clinical suspicion.
Does PSA increase with age?
Yes, largely because prostate volume increases with age.
Is a prostate biopsy always necessary?
No. The decision depends on clinical risk factors and imaging findings.
Bibliography
- Catalona WJ, Smith DS, Ratliff TL, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N Engl J Med. 1991;324:1156-1161.
- Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level ≤4.0 ng per milliliter. N Engl J Med. 2004;350:2239-2246.
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer. Lancet. 2017;389:815-822.
- Benson MC, Whang IS, Pantuck A, et al. Prostate specific antigen density: a means of distinguishing benign prostatic hypertrophy and prostate cancer. J Urol. 1992;147:815-816.
- Mottet N, Cornford P, van den Bergh RCN, et al. EAU Guidelines on Prostate Cancer. European Association of Urology Guidelines
- Bjurlin MA, Carroll PR, Eggener S, et al. Update of the standard operating procedure on the use of multiparametric magnetic resonance imaging for prostate cancer. J Urol. 2020;203:706-712.
- Schoots IG, Roobol MJ, Nieboer D, et al. MRI-targeted biopsy for prostate cancer diagnosis. Eur Urol. 2015;68:438-450.
- Carter HB, Albertsen PC, Barry MJ, et al. Early detection of prostate cancer: AUA Guideline. J Urol. 2013;190:419-426.