



Key points of the article
- Sexual impotence, or erectile dysfunction, is the inability to achieve or maintain an erection adequate for satisfactory intercourse.
- It affects about one in five men over 40 and can be a sign of general health problems, such as cardiovascular diseases.
- The mechanism of erection involves vascular, neurological, and hormonal systems, where nitric oxide plays a crucial role.
- The causes of sexual impotence include vascular, neurological, hormonal, and psychological factors.
- There are several effective therapies, including medications, injections, and prostheses, to treat sexual impotence.
What Is Sexual Impotence
Sexual impotence, medically defined as erectile dysfunction (ED), is the persistent or recurrent inability to achieve or maintain an erection sufficient for satisfactory sexual intercourse for both partners.
Table of Contents
- What Is Sexual Impotence
- Anatomy of Erection
- Penile Vascularization
- Mechanisms of Erection
- The Role of the Corpora Cavernosa in Erection
- The Role of the Nervous System in Erection
- The Role of Neurotransmitters in Erection
- The Role of Hormones in Erection
- Why Erectile Dysfunction May Develop
- Diagnosis of Erectile Dysfunction
- Treatments for Sexual Impotence
- Erectile Dysfunction and General Health
- When to Consult a Urologist
- Conclusion
- Bibliography
- You might also be interested in this article
It is a very common condition. Epidemiological studies indicate that about one in five men over the age of 40 experiences some degree of erectile dysfunction. The prevalence increases progressively with age, but the condition can also occur in younger men.
It is important to emphasize that erectile dysfunction is not simply a sexual disorder; it is often an early warning sign of more general health problems, particularly cardiovascular diseases, diabetes, or hormonal imbalances.
Today, thanks to advances in medicine, erectile dysfunction can be accurately diagnosed and effectively treated.
Anatomy of Erection
In simple terms, an erection is essentially the result of the ability to fill with blood two symmetrical elastic structures of the penis called the corpora cavernosa.
These structures are surrounded by an elastic membrane known as the tunica albuginea. Blood reaches the corpora cavernosa through the arterial system and drains through the venous system.
Erection occurs due to the compression of these veins, as will be explained later, resulting in reduced venous outflow and subsequent filling of the corpora cavernosa.
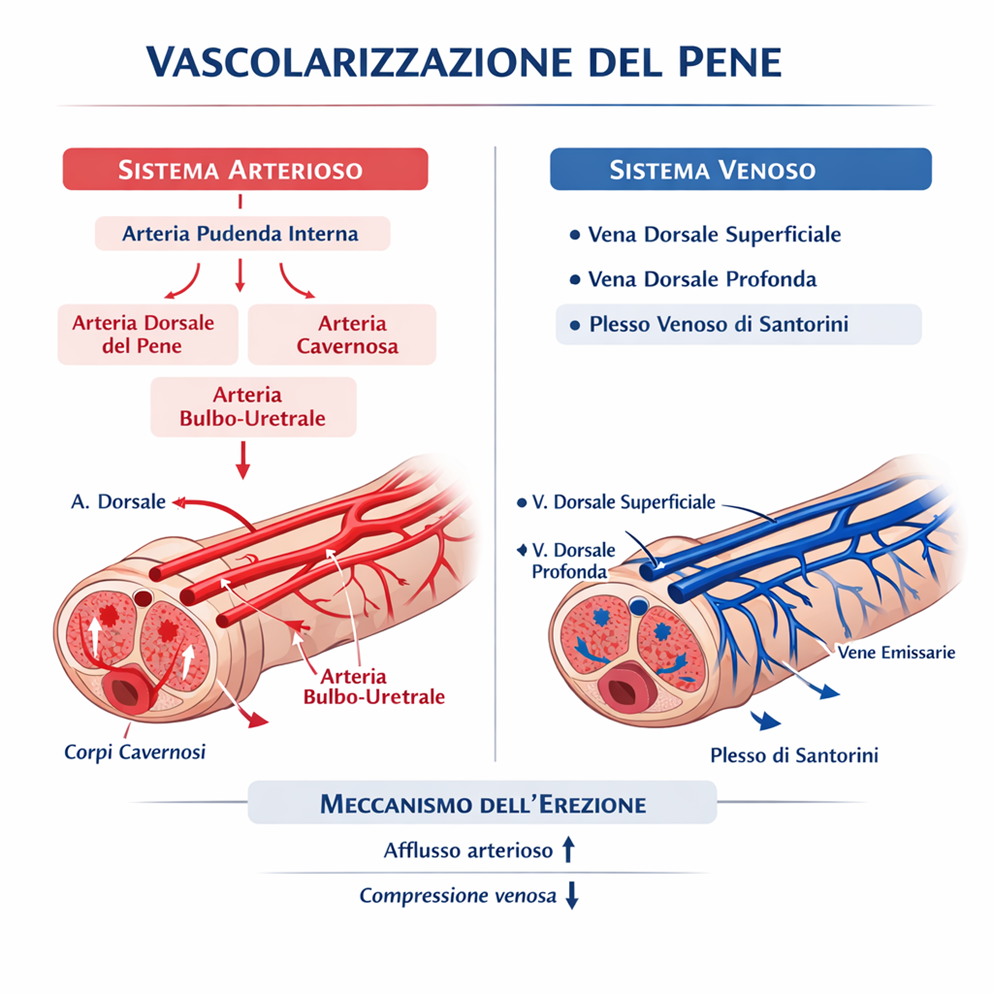
Penile Vascularization
Arterial System
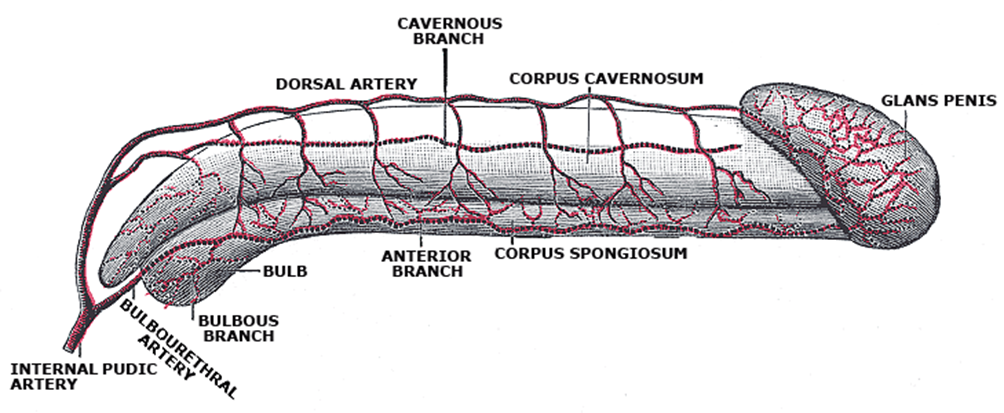
Blood supply to the penis originates from the internal pudendal artery, a branch of the internal iliac artery.
From this arise three main branches:
- Dorsal artery of the penis → supplies the skin and glans
- Cavernosal (deep) artery → responsible for erection
- Bulbourethral artery → supplies the corpus spongiosum and urethra
During erection, the cavernosal artery increases blood flow into the corpora cavernosa, leading to rigidity.
Venous System
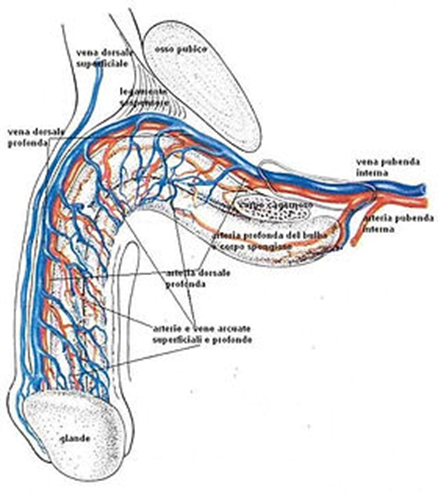
Venous drainage is divided into two systems:
- Superficial system → superficial dorsal vein → saphenous system
- Deep system → deep dorsal vein → Santorini’s venous plexus
The key mechanism of erection is the compression of the veins against the tunica albuginea, resulting in reduced venous outflow and maintenance of the erection.
Mechanisms of Erection
Erection is a complex phenomenon involving several systems of the body:
- brain and nervous system
- arteries and blood circulation
- penile cavernous tissue
- male hormones
- psychological and sensory stimulation
When a man receives sexual stimulation, the brain sends nerve signals that trigger the release of nitric oxide (NO) in the corpora cavernosa of the penis. This leads to:
- relaxation of penile smooth muscle
- dilation of the arteries
- increased blood inflow
- compression of the veins that normally drain blood
The result is increased penile rigidity, i.e., erection.
If any of these mechanisms is impaired, erectile dysfunction may occur.
The Role of the Corpora Cavernosa in Erection
At the basis of erection lies the integrity of the trabecular structure of the penile corpora cavernosa.
This structure forms the walls of the cavernous sinusoids, small vascular spaces through which arterioles and venules flow and where numerous nerve endings are present.
When this anatomical architecture is intact, the penis is able to rapidly fill with blood and achieve a full erection.
With advancing age, the trabecular structure may undergo degenerative changes that reduce the ability of the sinusoids to expand.
This process is one of the causes of the progressive decline in erectile function with age.
The Role of the Nervous System in Erection
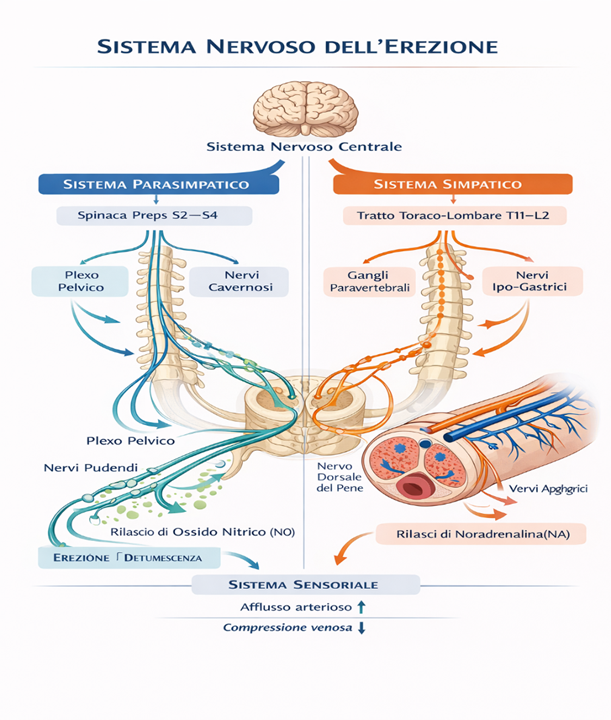
Erection is regulated by the autonomic nervous system, which controls the vascular mechanisms responsible for erection and subsequent detumescence.
Three main nerve centers are involved in the control of erectile function:
Cerebral Center
The primary center is located in the brain and includes:
- the paraventricular nucleus of the hypothalamus (PVN)
- the medial preoptic area
These brain structures integrate psychological, emotional, and sensory stimuli, contributing to what is known as psychogenic erection.
Spinal Centers
In addition to the brain, two centers located in the spinal cord are involved.
- The first is the thoracolumbar center (T12–L3), part of the sympathetic nervous system.
- The second is the sacral center (S2–S4), part of the parasympathetic nervous system.
From the sacral center arise nerve fibers that innervate not only the penis but also the bladder, prostate, and rectum.
Reflex Erection and Psychogenic Erection
Stimuli from sensory receptors in the genital area reach the spinal centers and can generate a reflex erection.
Through ascending spinal pathways, these signals subsequently reach the brain centers, allowing conscious perception of sexual stimulation.
The neural pathways regulating erection are bidirectional:
- Sensory stimuli from the penis can trigger reflex erections at the spinal level.
- Psychogenic stimuli originate in the brain and are transmitted to the thoracolumbar and sacral spinal centers.
This explains why erection can be influenced by both physical stimuli and mental or emotional factors.
The Role of Neurotransmitters in Erection
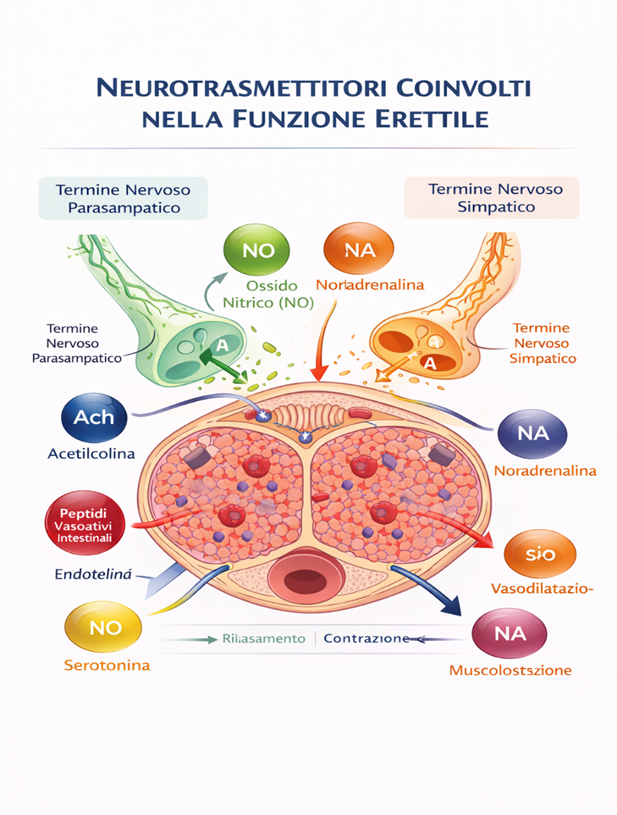
The transmission of nerve impulses that regulate erection involves several neurotransmitters, including:
- dopamine
- serotonin
- oxytocin
These mediators act on three main neuro-effector systems:
- adrenergic system
- cholinergic system
- non-adrenergic / non-cholinergic system
At the local level, other substances are also involved in regulating the tone of the smooth muscle of the corpora cavernosa, such as:
- nitric oxide (NO)
- endothelin
- prostaglandin PGE1
The Role of Hormones in Erection
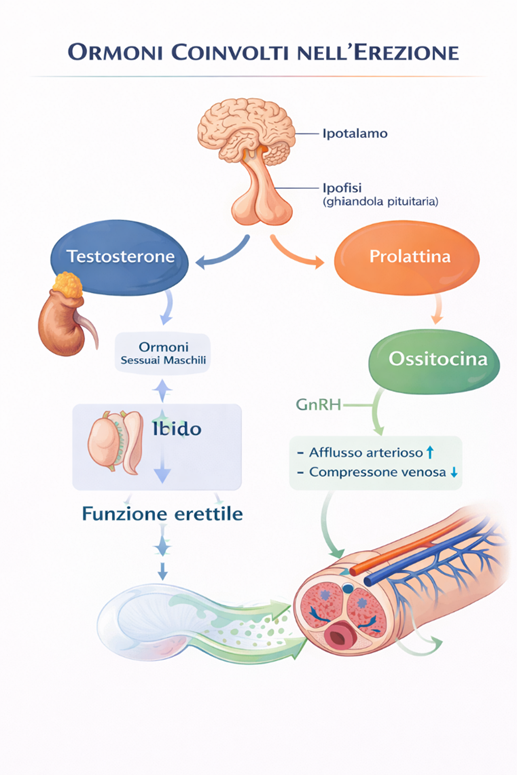
The hormonal system is also essential for male sexuality.
Among the most important hormones are:
- gonadotropins (FSH and LH)
- testosterone
- dihydrotestosterone
- SHBG (Sex Hormone Binding Globulin)
Androgens are essential for the development of male sexual characteristics, but they also play an important role in maintaining libido and erectile function.
A reduction in testosterone levels may contribute to erectile dysfunction and decreased sexual desire.
Why Erectile Dysfunction May Develop
Erectile dysfunction can occur when one or more of the mechanisms described above are impaired.
Vascular Causes
Penile arteries are very small and may be affected by atherosclerosis before the coronary arteries. For this reason, erectile dysfunction is often considered an early warning sign of cardiovascular disease.
In many cases, erectile dysfunction appears 3–5 years before a cardiac event.
The most common causes are vascular, meaning related to blood circulation. Main risk factors include:
- atherosclerosis
- arterial hypertension
- diabetes
- high cholesterol
- cigarette smoking
- obesity
- metabolic syndrome
Neurological Causes
The nervous system controls the erection mechanism. Certain diseases or injuries can interfere with the nerve signals necessary for erection.
Main neurological causes include:
- diabetic neuropathy
- multiple sclerosis
- Parkinson’s disease
- spinal cord injuries
- pelvic surgery
An important example is radical prostatectomy for prostate cancer, which may damage the erectile nerves.
Hormonal Causes
Possible hormonal causes include:
- hypogonadism
- increased prolactin levels
- thyroid disorders
The main hormone involved in male sexual function is testosterone. Low testosterone levels may cause:
- reduced sexual desire
- erectile difficulties
- fatigue and loss of energy
However, testosterone deficiency represents a less frequent cause compared to vascular problems.
Psychological Causes
In younger individuals, erectile dysfunction may have a predominantly psychological origin. Common causes include:
- performance anxiety
- stress
- depression
- relationship problems
- fear of inadequacy
A psychological vicious cycle often develops: a single episode of erectile difficulty generates anxiety, which further worsens the problem.
Medications and Substances
Some medications may interfere with erectile function. Among the most involved:
- antidepressants
- antihypertensive drugs
- diuretics
- antipsychotics
Additionally, the following may contribute to erectile dysfunction:
- smoking
- alcohol abuse
- marijuana/hashish
- cocaine
- heroin
- other drugs
Diagnosis of Erectile Dysfunction
Diagnosis is made by a urologist or andrologist through a structured clinical evaluation.
Medical History
The first step is collecting detailed information about the problem:
- duration of symptoms
- whether the erection is absent or only reduced
- presence of spontaneous nocturnal erections
- presence of conditions such as diabetes or hypertension
- medications being taken
A commonly used questionnaire is the IIEF-5 (International Index of Erectile Function).
Physical Examination
During the urological examination, the following are assessed:
- penis and testicles
- presence of anatomical abnormalities
- blood pressure
- body weight
- signs of hormonal deficiency
Blood Tests
The most useful tests include:
- blood glucose
- cholesterol
- testosterone
- prolactin
- thyroid hormones
These tests help identify possible metabolic or endocrine causes.
Dynamic Penile Color Doppler Ultrasound
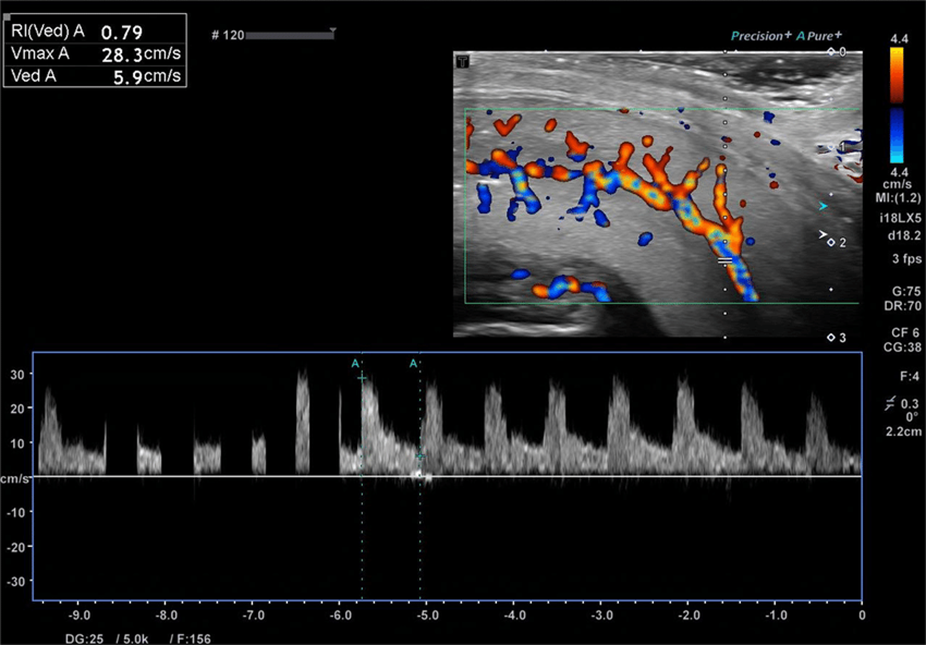
One of the most important tests in the diagnosis of sexual impotence is the dynamic penile color Doppler ultrasound. This examination allows the evaluation of:
- penile arterial blood flow
- possible circulatory problems
- the presence of venous leakage
It is particularly useful in young patients or when a vascular cause is suspected.
Treatments for Sexual Impotence
Today, several effective therapies are available for sexual impotence. The choice depends on the underlying cause of the problem and the patient’s characteristics.
Lifestyle Changes
The first step is to correct risk factors. Main recommendations include:
- quitting smoking
- engaging in regular physical activity
- losing weight
- controlling diabetes and blood pressure
- limiting alcohol intake
These changes can significantly improve erectile function.
Medications for Erection
The most commonly used therapy for sexual impotence consists of phosphodiesterase type 5 inhibitors (PDE5 inhibitors). The most well-known include:
- sildenafil
- tadalafil
- vardenafil
- avanafil
These drugs improve blood flow to the penis and facilitate erection. Their effectiveness is high, with success rates in 70–80% of patients.
It is important to remember that they work only in the presence of sexual stimulation.
Intracavernosal Injections
When oral medications are not effective, intracavernosal injections of vasoactive drugs, such as alprostadil, can be used.
The injection induces a direct pharmacological erection and can be highly effective.
Vacuum Devices
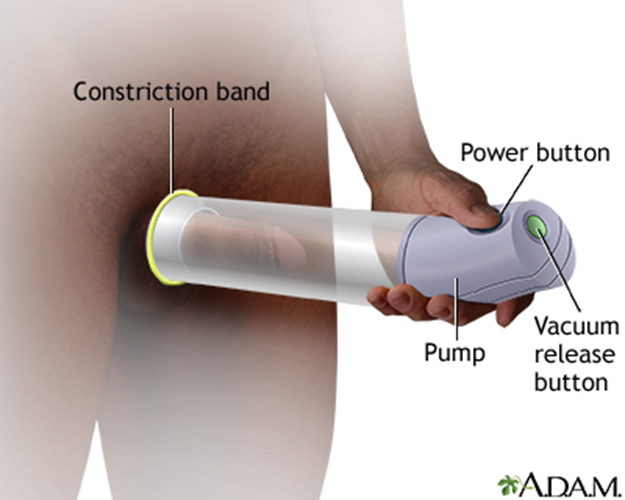
The vacuum device creates negative pressure around the penis, promoting blood inflow. Subsequently, an elastic ring maintains the erection.
Penile Prosthesis
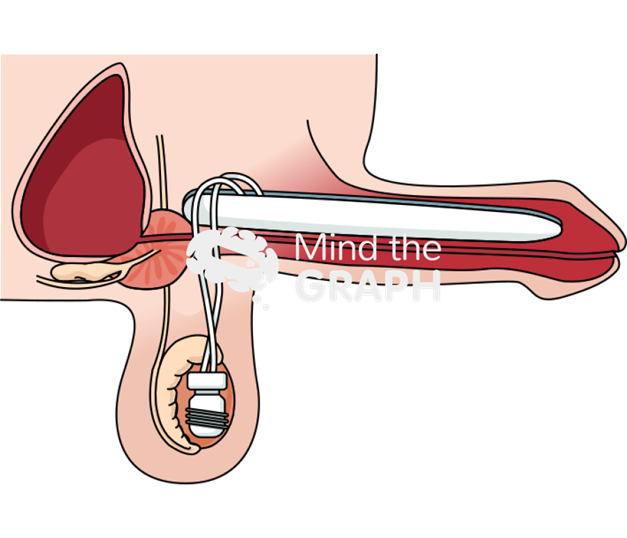
In more severe cases or when resistant to other therapies, penile prosthetic surgery may be considered.
The most modern prostheses are hydraulic and inflatable, allowing a very natural erection. Patient satisfaction exceeds 90%.
Erectile Dysfunction and General Health
Today we know that erectile dysfunction may represent an important indicator of cardiovascular health. For this reason, the onset of sexual impotence should always be evaluated by a specialist.
Early identification of the problem often allows the diagnosis and prevention of cardiovascular diseases.
When to Consult a Urologist
It is advisable to consult a specialist when:
- erectile difficulties last more than 3 months
- the problem appears suddenly
- conditions such as diabetes or hypertension are present
- erectile difficulties cause stress or relationship problems
A specialist evaluation helps identify the causes and choose the most appropriate treatment.
Conclusion
Erectile dysfunction is a very common but often underestimated condition.
Today, medicine offers advanced diagnostic tools and numerous effective treatments that allow the problem to be resolved in most cases.
Openly discussing the issue with a specialist is the first step toward restoring a satisfying sexual life and improving overall quality of life.
Bibliography
- Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. Journal of Urology. 2018.
- Salonia A, Bettocchi C, Carvalho J, et al. EAU Guidelines on Sexual and Reproductive Health. European Association of Urology. 2023.
- Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates. Journal of Urology. 1994.
- Montorsi P, Ravagnani PM, Galli S, et al. The artery size hypothesis. European Heart Journal. 2005.
- Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. New England Journal of Medicine. 1998.
- Corona G, Isidori AM, Aversa A, et al. Endocrinologic control of male sexual function. Journal of Sexual Medicine. 2016.
- Miner M, Parish SJ, Billups KL, et al. Erectile dysfunction and cardiovascular disease. Mayo Clinic Proceedings. 2019.