(From the 2010 Guidelines of the European Society of Urology)
Cystitis - Medical
Interstitial Cystitis (or, as defined by the International Continence Society, Painful Bladder Syndrome), unfortunately evokes apocalyptic scenarios, strengthened by the infinite testimonies of patients who are afflicted by it. Fortunately, most patients who fear they are ill with I.C. they are absolutely not but they usually suffer from chronic cystitis or Chronic Pelvic Floor Pain Syndrome.
For those who don't know, we would like to point out the existence of a specific, very active company that deals exclusively with this disease (www.aicionlus.org).
DEFINITION
The definition of interstitial cystitis – C.I. o PBS (Pain bladder syndrome) is the following: Presence of pelvic pain referable to the bladder, which is exacerbated with filling of the same, accompanied by urgency and increased urination frequency during the day and night, lasting for more than six months and is not associated with urinary infections (Neurourol Urodyn. 2009;28(4):274-86).
The statistical incidence of the disease varies enormously in the literature from publication to publication. This depends on the fact that many works, especially in the past, have taken into account, in making the diagnosis, only the symptoms complained of by the patient, without carrying out the standardized clinical tests required today (See below). Furthermore, and this is very important to underline, these statistics vary from country to country. In fact, there are countries where the high incidence of the disease may depend on specifically environmental factors, such as for example in Finland where a 2005 research (J Urol 2005;174,2:581-583) highlighted the presence of 530/ 100,000 patients affected by IC. For the Italian population, the statistics recorded in Austria in 2007 are more applicable (Eur Urol; 2007; 51.3:803-808) which document an incidence of the disease in 306/100,000 with peaks of 464/100,000 in middle-aged women . The disease in fact affects almost exclusively women with a predominance over men of 10:1 and with a preference for those of the Caucasian race (Europeans).
DIAGNOSIS
(AUA guidelines 2011)
Basic diagnosis principles: history, physical examination, laboratory tests to exclude other similar pathologies (see below). According to the opinion of the experts of the American Urologic Association, cystoscopy and urodynamic examination are useless in cases where the type of symptoms is striking. However, these two investigations remain appropriate when, after the basic evaluations, the diagnosis remains in doubt. Potassium sensitivity testing should not be used in primary care as its result may change both the direction and approach of clinical treatment.
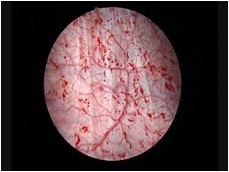
Fig.1
AUTOMATIC INCLUSION CRITERION (Fig.1):
Appearance of Hunner's ulcer on hydrodistention (present in less than 10% of patients)
INCLUSION CRITERIA (Fig.2):
Fig.2Bladder pain upon filling which eases with emptying (reason for urination frequency).
Pain (suprapubic, pelvic, urethral, vaginal or perineal).
Glomerulation (appearance of haemorrhagic petechiae) during hydrodistention (90% of patients).
Poor tolerance of hydrodistension.
The characteristics of IC pain are the key symptom of the disease:
It is correlated with the degree of bladder distention.
It is located in the suprapubic area with possible irradiation to the groins, vagina, rectum or sacrum.
It fades with bladder emptying but returns soon after.
EXCLUSION CRITERIA:
Age below 18 years
Malignant or benign neoplasms of the bladder
Uterine, cervical, vaginal or urethral neoplasm
Postactinic cystitis
Tuberculous cystitis
Current bacterial cystitis
Concomitant bacterial or fungal vaginitis
Cyclophosphamide cystitis
Symptomatic urethral diverticulum
Active genital herpes
Bladder or urethral stones
Daytime urination frequency less than 5 times in 12 hours
Nocturnal urination frequency less than 2 times
Improvement or disappearance of symptoms with antibiotics, urinary antiseptics, analgesics
Duration of less than 12 months
Presence of overactive bladder (on urodynamic examination)
Bladder capacity greater than 400 cc. in the absence of urinary urgency.
Therefore we remember that the diagnosis of interstitial cystitis becomes very convincing according to Ottem (Urology 2005;66(3):494-99) with:
Cystoscopy with hydrodistention for 1-3 minutes with 100 cc of water.
Appearance of petechial hemorrhages in at least 3 bladder quadrants.
Presence of at least 10 petechiae per quadrant.
Bladder biopsy
Regarding the appearance of glomerulations (petechiae), we remind you that it is variable and its absence can erroneously lead to excluding the diagnosis of IC. Furthermore, remember that glomerulations can be detected in irradiated bladders, in defunctionalized bladders, in bladder cancer, in exposure to chemotherapy and also, albeit rarely, in normal bladders.
However there are other signs of probability, such as:
Presence during the urodynamic examination of reduced bladder capacity, with urgency appearing at less than 150cc.
Pain upon intravesical instillation of potassium solution (in 75% of patients). It has been hypothesized that positivity to this test is positively predictive for response to treatment with GAGs (Gupta; BJU Int 2005;96(7):1063-66).
The bladder biopsy in the EAU guidelines is not pathognomonic, but is considered to support the diagnosis if the presence of mast cells is highlighted (Nordling; Eur Urol 2004;45(5):662-69).
PATHOGENESIS
There are many different hypotheses about the causes of IC.
1) Infections: despite the use of very sophisticated searches for bacteria (including Helicobacter Pilorii) or viruses, no pathogenic microorganisms have ever been found.
2) Inflammation: it is considered an essential part of the disease, associated with pancystitis and perineural infiltrates of lymphocytes and plasma cells. But it is probably to be considered an effect and not a cause.
3) Activation of Mast Cells: remember that mast cells are immuno cells containing strongly pro-inflammatory factors such as histamine, serotonin and cytokines. In bladder biopsies, as mentioned above, there can be a 10-fold increase in mast cells (Peeker; J Urol 2000; 163(3):1009-15).
4) Endothelial dysfunction with GAGs defect: all patients with I.C. present fragility or lesions of the endothelium which manifest themselves with fissures or ruptures of the endothelium upon hydrodistention and subsequent appearance of petechiae. The increase in the level of sulfated GAGs in patients with more severe symptoms is considered by some to be a marker to monitor the evolution of the disease (Lokeshwar; J Urol 2005;174(1):344-49).
5) Alteration of autoimmunity: since 1970, multiple studies have been carried out on autoantibodies during C.I. However, the results are still inconclusive.
6) Alteration of nitric oxide metabolism: also in this case the results were inconclusive, although the level of evaporation of nitric oxide in the urine of patients with IC. is significantly higher than in control groups (Logadottir; J Urol 2004;171(3):1148-50).
7) Neurobiological hypothesis: in patients with C.I. an increase in sympathetic innervation is detected with an increase in neurotransmitters. Therefore, it is widely assumed that this is the start of the cascade of events that lead to the full-blown disease.
8) Toxic substances: the presence of acidic or aggressive substances in the urine, in the presence of lability of the endothelium, can probably trigger a decline in the mucosal defenses.
9) Hypoxia: it has been observed that there is a decrease in the density of capillaries in the subendothelium in the presence of C.I. This situation of hypo vascularization could lead to a decrease in wall oxygenation. Following this hypothesis, in fact, remissions of the disease have been achieved with hyperbaric therapy sessions (Pontari; J Urol 1999;162(2):330-34).
11) Increase in NGF (Nervous Growth Factor): In a recent work by Evans and Moldwin it has been demonstrated that in interstitial cystitis there is an increase in NGF in the urine and in the interstitium which participates in inflammatory conditions, generating and maintaining the pain. And it has also been possible to demonstrate (see new therapies) how blocking NGF reduces the symptoms of bladder hyperactivity, one of the sequelae of IC.
10) Interaction of multiple factors: this is the most current hypothesis, which sees the multiple interaction between the immunological, nervous and endocrine systems as the cause.
THERAPY
According to the recommendations of the American Urologic Association, there are six levels of therapeutic intervention
The first level is based on:
Principles of clinical education (knowledge of bladder anatomy and physiology, explanation of the disease and its therapeutic options) Principles of "self-wellbeing" (modification of behaviors that can cause symptoms, management of stressors that exacerbate disorders)
The second level is based on:
Manual physical therapy with maneuvers that resolve pelvic and abdominal pain and/or release trigger points (avoid stretching exercises and have the maneuvers performed by specifically trained clinicians).
Oral therapy (in alphabetical order) with Amitriptyline, Cimetidine, Hydroxyzine, Pentosanpolysulfate, Pregabalin.
Intravesical therapy (in alphabetical order) with Ac. Hyaluronic+Chondroitin sulfate (Hyaluryl), Heparin, Lidocaine.
The third level is based on:
Cystoscopy + hydrodistension (under anesthesia, with low pressures and short duration).
Laser or local fulgurations or cortisone infiltrations in the presence of Hunner's ulcers.
The fourth level is based on:
Neurostimulation with a permanent implant, if the temporary implant was effective and previous therapies were unsuccessful.
The fifth level is based on:
Oral administration of Cyclosporine. Intradetrusor infiltration of botulinum toxin A (with the possibility of bladder paralysis and consequent intermittent catheterizations).
The sixth level is based on:
Bladder surgery with replacement cystoplasty or urinary diversion with or without cystectomy (only in ultra-selected patients and when any other therapy has failed to control symptoms and maintain a minimum sustainable quality of life).
EXPERIMENTAL TREATMENT OUTSIDE THE AUA GUIDELINES
(Evans et al: J of Urol. ol.185:1551-52, May 2011).
As already reported, it has been demonstrated that nerve growth factor (NGF) directly participates in the inflammation of the bladder wall and generates and maintains chronic pain. Also in animals suffering from interstitial cystitis and with high levels of urinary excretion of NGF, blocking this factor immediately reduced its hyperactivity. Starting from these premises, Evans conducted a randomized double-blind study in 2011, administering to patients with C.I. TAMEZUMAB which is a monoclonal anti-NGF antibody. The results of the study were that Tamezumab was very effective in treating painful symptoms, but did not reduce urinary frequency or increase the amount of urine voided per single urination.
THERAPEUTIC BEHAVIORS TO AVOID:
Prolonged administration of antibiotics
Prolonged administration of cortisone
Intravesical instillation of the Calmette-Guerin bacillus
Intravesical instillation of Resiniferatoxin
Hydrodistension at high pressures or with long times (greater than 10 minutes).
Therefore in Conclusion:
It is necessary to start with the most conservative treatments possible and reserve surgery for the most resistant situations or for those with the presence of Hunner's ulcers The initial level of treatment depends on the doctor's judgment, the severity of the symptoms, and the patient's wishes Multiple treatments can be considered in the patient's best interest Ineffective treatments must be discontinued before moving to a different level of intervention Pain management must be the primary goal of any treatment In the absence of results you must always be ready to reconsider the diagnosis